Apart from shortness, vegephobia and addiction to technology, how are children different?1
This talk focuses on what areas of child development are affected by abuse and neglect, how central the notion of attachment is to child development, and how clinicians plan assessments of what parents may offer. It integrates some of my more technical papers used to train clinicians.
Serious Question: Why are child abuse and neglect bad?
[18-2000] Attachment
An attachment relationship is the fruit of early childhood development, meaning that a child has been well cared-for, and a consistent caregiver, or a few consistent caregivers, have effectively responded to his or her needs. In well functioning families, the baby decrees what should be done and the caregiver learns to interpret and meet these needs. A “good enough” mother is sensitive and flexible in the way she studies and reacts to her baby, and intuitively learns how to supply what is required.
In this safe, predictable environment the primary caregiver can become a “secure base” for the child. The child knows the mother is there to provide security when it is required, so that he or she can then safely learn about the world through personal exploration. A baby brought up in this secure, nurturing environment learns to expect relationships to be reciprocal and direct. A signal from one person leads to a straightforward response from the other.
From this start, these children are more likely to learn that the world behaves according to intelligible principles, they will expect rewarding relationships based on assertiveness and empathy, they are comfortable with bodily contact, and will be predisposed to enjoy school and other learning activities.
For a human baby, born the most vulnerable of species, it is highly dangerous to be unattended, or not responded to appropriately. Babies are built, both biologically and psychologically, to engage with, and elicit care from others. The caregivers who make them most comfortable are those who are stronger, wiser, safer and irrationally interested in their welfare. Naturally, a primary, predictable caregiver, usually in the form of a mother, often manages to fulfil these demanding occupational criteria.
Home should be the safest of places, yet we know that for some people home is the place of greatest danger. How do people manage to survive in some homes? When the mother does not respond to the baby’s cues (eg eye contact, crying, physical movements), the baby has to adapt differently. Infants need to adapt to dangerous family experiences by using the “anxious” strategies of “defended” (usually seen as a “Type A insecure” or “avoidant” strategy) or “coercive” (or “Type C insecure” or “ambivalent”) attachments. Crittenden (2008) regards these anxious attachment strategies as inherently adaptive, in that they protect the infant, and help unresponsive caregivers to be forced to meet these needs.
| Development area | A child needs … | Impact of child abuse and neglect |
|---|---|---|
|
Physical development (Prevention of injury, freedom from preventable illnesses and chronic conditions. Nutrition, sleep, dental care, gross and fine motor skills.) |
Physical care and safety Consistent safety from physical and sexual abuse and from exposure to domestic violence, in placements and contact visits; also consistent hygiene, supervision, housing, food, clothing, sleep, rest, health care, continuity, routine, advocacy, etc. |
Problems begin in pregnancy (see below)
As adults: |
|
Emotional development (Ability to regulate emotion, to feel safe, develop self-efficacy) |
Empathic attention This is at the core of the attachment relationship. The child needs someone to show interest, compassionate understanding, and to respond effectively to his or her emotional needs, feelings and thoughts. |
|
|
Attachment relationship This is the focus of a young child’s emotional and social development, providing the core his or her affect regulation, self-knowledge, trust and capacity to learn. Children need to feel safe, to settle, to develop a sense of self, and to know that their needs will be responded to. This requires an ongoing commitment from consistent caregiver(s), who offer responsive caregiving, empathic attention, acceptance of the child as an individual, and a model for self-concept and social learning. This is also the foundation for establishing autonomy and individual identity. |
As adults, greater risk of: |
|
|
Behavioural development (Impulse control, self-care skills, independent behaviour) |
Emotional and behavioural self-regulation This involves learning how to recognise and manage impulses and feelings, how to express them appropriately, how to get needs met effectively and safely, and how to respond appropriately to others. To achieve this requires effective limit-setting and discipline. |
|
|
Social development (good attachments, theory of mind, capacity to interpret and trust others, interpersonal skills, peer relations, personal identity, understanding and enhancing one’s role in society) |
Role model(s) A child learns by copying the behaviour of others, with the end result of learning how to play a constructive, independent social role and how to participate in the range of social relationships necessary for human society, from the intimate through to formal citizenship roles. This implicit, behavioural learning requires continuity of social modelling, facilitating the adoption of pro-social values, leading to a sense of meaning, belonging and cultural identity. |
Speech and language development problems10
|
|
Cognitive and cultural development (Play, language, problem-solving, reading, educational achievement, love of learning, creativity, cultural identity) |
Cultural education One of the main tasks of childhood is to learn the wider explicit skills needed to adapt successfully to a complex modern community. These include language and communication, reading, transport, financial, health, occupational, recreational, cultural and spiritual education, leading to sense of personal identity in the context of human society and one’s own meaningful values in life. Cultural educational needs and learning styles expand and widen over time from the family hearth to the wider society. They are acquired by different learning styles, from observation, stimulation/interaction, exploration/learning, socialisation, play opportunities, and formal instruction, through to participation in school, sport, cultural, workplace and spiritual milieus. |
|
Early development from the abused child’s perspective:11
- (i)
-
You will have more difficulties and complications in pregnancy.
- (ii)
-
The first abuse is usually in utero, from one of the mother’s partners.
- (iii)
-
You have 2–4 times greater risk of prematurity or being underweight.
- (iv)
-
You are 10 times more likely to be delivered by Caesarean section.
- (v)
-
You are likely to be a disappointment to your mother.
- (vi)
-
The normal symbiotic relationship is missing.
- (vii)
-
Your needs are not met with alacrity and concern.
In other words, child abuse and neglect can affect every area of a child’s health, development and potential. The challenge for Children’s Court Clinic clinicians is to understand what are the needs and resources, and the developmental risks and strengths, for each particular child.
Child development12
Children who are neglected may be delayed in all areas, but it is common for them to have normal gross motor milestones, and delayed language and social development.
| Consensus | Down kiddies | |
|---|---|---|
| Gross Motor | ||
| Roll over | 5 m | |
| Sit alone | 7(5–9) m | 11 m |
| Crawling (creeping) | 10 m | 15 m |
| Stand alone | 11 m | 20 m |
| Walk alone | 11–15 m | 26 m |
| Run | 19–24 m | |
| Climb stairs (crawling) | 15 m | |
| — up alternating feet | 3 yrs | |
| — down alternating feet | 5 yrs | |
| Language | ||
| Turn to mother talking | 6 m | |
| First laugh | 2–6 m | |
| “Dada” or “Mama” | 10 m | |
| 1st words (not imitating) | 12 m | 23 m |
| 2 words together | 20 (19–22) m | 3 yrs |
| Personal-Social | ||
| Finger feeding | 9–10 m | 18 m |
| Drink from cup | 12–13 m | 23 (12–32) m |
| Feed self with spoon | 14–18 m | 29 m |
| Dry during the day | 18 m–2 yrs | |
| Dry at night | ~ 3 yrs | |
| Play | ||
| Play independently on floor | 4–6 m | |
| “Peekaboo” | 9 m | |
| Parallel play | 21–27 m | |
| Cooperative play with peers | 4–5 yrs |
Parenting and development
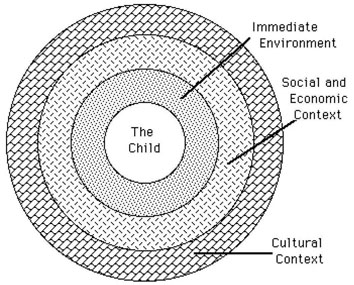
Human development is not individual, but social. Bronfenbrenner’s social-ecological model of development (1979) describes these influences as intercultural, community, organisational, and interpersonal or individual. He saw the individual, organisation, community, and culture to be nested factors, like Russian dolls. Each echelon operates fully within the next larger sphere.
Risks to children tend to be cumulative, but attachment is the central focus. Peter Fonagy (1998) reviewed relevant developmental factors in relation to a vulnerable population of infants. He categorised risk and protective factors within early development, as linked to social inequalities:
- 1.
-
Biological factors (attenuated by psychosocial interventions)
- 2.
-
Family and social factors (Low SES, deprivation, family instability, single parenthood, maltreatment)
- 3.
-
The quality of parenting (including differential sibling effects, parental psychopathology)
- 4.
-
The quality of attachment status (attachment security correlates with SES)
- 5.
-
The influence of non-maternal care (for children of insensitive mothers who were in low quality care).
He concluded that the relationship with the caregiver is arguably the most important mediator of the impact of social inequalities on early child development. This view is strongly supported by Schore’s (2003) review of more recent research, which concluded that social stressors related to attachment or “relational” trauma, whether abuse or neglect, can lead to severe affect dysregulation and have “more negative impact upon the infant brain than assaults from the nonhuman or inanimate, physical environment” (ibid, p 237).
The social ecological model considers behaviour from the perspective of continuous interactions within nested systems, from individual, interpersonal, organisational, community, through to intercultural factors. In our child development focus these systems might be from the maternal dyad, father and sibling relationships, extended family and kinship group, family friends, school, neighbourhood, friends, church or sporting groups, work or shops, through to public services and federal elections. Over time, development occurs through widening ripples through these areas.
The family must also interact constructively with the extended family and neighbourhood, allowing the child to learn citizenship, safe behaviour and how to live independently in a human community. In a very practical sense it is important for the family to facilitate the child’s independence and learning at school, to make effective use of health and medical services, and to develop constructive peer relationships.
Characteristics of abusive parents and their children
The NSW Child Deaths Committee (2000) raised specific concerns when a parent is drug-affected, particularly by methadone, and if the child is aged less than 12 months. Parental abuse of alcohol and other drugs has contributed to children’s deaths from dehydration, pneumonia, bronchiolitis, toxicity, drowning and motor vehicle accidents. It is also associated with social isolation, poverty, domestic violence, parental mental illness, parental personality disorder, single parenthood with serial partners, inadequate support networks, criminal activity and involvement in drug-using networks.
The Denver Group (Steele and Pollock, 1974) identified characteristics of abusive parents:
- (a)
-
Immature and dependent
- (b)
-
Socially isolated
- (c)
-
Poor self-esteem
- (d)
-
Difficulty seeking or obtaining pleasure
- (e)
-
Distorted perceptions of the child (including role reversal)
- (f)
-
Fear of spoiling the child
- (g)
-
Belief in the value of punishment
- (h)
-
Impaired ability to empathise with the child’s needs and to respond appropriately.
Crittenden, 1988, found:
- (a)
-
In abusive families, children were described as:
- (i)
-
Difficult and acting out, or wary, compliant and inhibited.
- (b)
-
In neglecting families they were described as:
- (i)
-
Very passive in infancy
- (ii)
-
Sometimes very active when older
- (iii)
-
Having a limited ability to attend to others
- (iv)
-
Having “significant developmental delay”.
- (c)
-
In “abusing and neglecting families”, children were described as:
- (i)
-
Being out of control
- (ii)
-
Unable to learn to manage their parents as can abused children
- (iii)
-
Unable to safely ignore their parents (as neglected children can)
- (iv)
-
Having numerous intellectual, physical and behavioural anomalies.
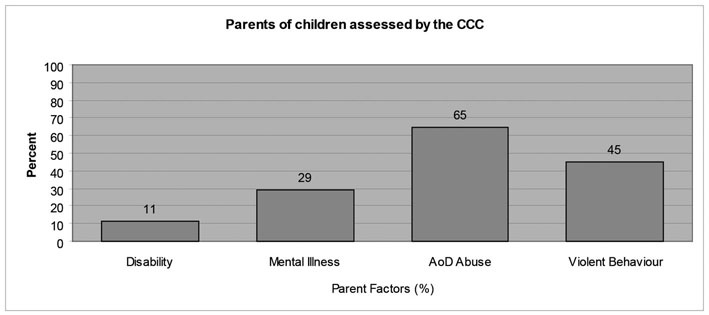
A snapshot from clinic data
A recent review 14of some Authorised Clinicians’ reported summaries of their findings found high levels of disability (broadly defined), alcohol and other drug misuse, violent behaviour problems and mental illness for the parents of the at-risk children.
There is no such thing as a child, and no such thing as a parent
I hope this summary has shown why it is not possible to assess either a child or a parent alone. Each needs to be understood in relation to the other. My model of assessment of parenting capacity15, from which the following information is drawn, attempts to allow the interactions between the child’s needs and the parents’ resources to be considered. It is based on considering the parenting dimensions that relate to these needs (Steinhauer 1991, Mrazek et al, 1995, Brennan 1996, Azar et al, 1998).
Stafford and Zeanah (2006) have summarised the essentials of parenting as involving the provision of sustenance, stimulation, support, structure and surveillance. We need to operationalise what these may mean, particularly for vulnerable children.
Assessments of parenting capacity need to reflect the fact that the majority of carers are women (Wyndham 2008). When separated fathers are assessed for parenting capacity, it is often their new partners who are expected to do the work.
- (i)
-
Responsive caregiving and protection
This includes the flexible yet continuous use of basic childcare skills, without which child development is seriously at risk:
-
Adequate physical care, using appropriate routine skills (feeding, clothing, toileting, cleaning, bedtime) adapted to the situation at hand;
-
Awareness of the particular child’s developmental needs, and the ability to meet them, including child care and medical emergencies;
-
Capacity to protect the child from physical danger in the home and neighbourhood, from physical or sexual abuse, and from exposure to domestic violence, and from potential danger from others in the household and the wider social network.
Drug use, mental illness, intellectual disabilities and personality disorders may limit these skills.
-
- (ii)
-
Reflective function
Donald and Jueridini (2004) have clarified recent research’s emphasis on the importance of practical parental empathy, involving the “capacity to see the experience from the child’s point of view, and to realistically appraise what might need to change for the child to thrive in their care”. Steinhauer (1991) has defined this more specifically as “responsive caregiving”.
Fonagy (2000) has found social cognition to be a key mediator of the impact of attachment. Parents’ ability to reflect or mirror (before their child’s birth), or their reflective function helps predict their child’s attachment security (at 18 months). It enables:
-
Sensitive reflection by the caregiver, allowing the child to internalise a representation of its mental state (“So this feeling I’m having is what Mum calls anger”, etc);
-
The child to feel safe in exploring the parent’s mind to understand feelings and thoughts that account for their behaviour;
-
Play to be facilitated, which helps a child move from a subjective world where internal experience and external reality are assumed to be equivalent, to a mentalised internal world, where subjective experiences are recognised as but a version of external reality.
Reflective function predicts the transmission of attachment styles better than parental sensitivity, genetics or behavioural modelling.
These experiences help the child develop an intentional stance, the ability to understand others’ mental states (thoughts, beliefs, feelings, desires), to make sense of and predict their actions. The hallmark of achievement of this stance is the child’s recognition that a person’s behaviour may be based on a mistaken belief (3–4 years). Our social maturity, and capacity for empathy and rapport, depend on our ability to understand the mental world of another person.
-
- (iii)
-
Bonding
This typically means the parent’s attachment or emotional commitment to the child:
-
Emotional acceptance of the child
-
Responsibility, commitment (time, energy)
-
Relationship continuity
-
Warmth rather than rejection/hostility (overt, covert neglect and/or abuse)
-
Management of traits attributed to the child and competition for attention from partner/spouse.
A parent needs to “be there” emotionally and physically for the child, rather than absorbed solely by his or her own, a partner’s, or another child’s needs. Wyndham (2008) has reminded me that this can be assessed partly by the way parents speak of their children. The words they use to describe the children, (eg ”a little liar”, ”she’s manipulative”), and the tone and manner in which they speak of them reveal parental attributions, expectations and understanding of child development. It is also relevant to consider to what extent the parent sees the child as a narcissistic extension of him- or herself.
-
- (iv)
-
Emotional availability
A parent’s capacity to regulate his or her own emotional tension leads to a capacity to understand and respond to the child’s emotions, and to treat the child as a real, independent human entity. This can be limited by psychiatric or personality disturbance (depending on type, severity, and affected by ability to use clinical interventions). Emotional availability may be aided by supports for the parent and the management of stress from a possibly adverse environment (parent relationships, climate at home, extended family and social supports, employment, financial security). Bretherton (2000) reports a variety of studies closely linking maternal sensitivity in terms of emotional availability with attachment quality in infancy and maternal “states of mind” revealed by the AAI.
- (v)
-
Strategic Behaviour Management
This includes acceptance of supervisory responsibilities, knowledge of various child management strategies, and the ways of selecting, applying and adapting them appropriately for different situations with children. It will require developmentally appropriate expectations and a capacity to analyse a particular situation, including limit setting, redirection, discipline, flexibility and support for the child’s autonomy.
Some of these skills can be taught, for example in 1-2-3-Magic, Triple P, Parent Effectiveness Training or Systematic Training for Effective Parenting. A parent also needs to be perceptive, sensitive and relatively consistent in using them. The child needs to be able to learn how to overcome unhelpful habits, control impulsiveness, develop assertiveness skills, negotiation, conflict resolution and other effective ways of behaving.
- (vi)
-
Ability to transmit the community’s cultural values
One of the main roles of a parent is to help the child to learn how to relate to other people. The family is the place to learn safely how to cooperate, compete, communicate and participate in society. In helping children to learn how to participate effectively and independently in the wider culture, a parent will both consciously and implicitly train the child in how to behave, passing on practical knowledge about ethics and cultural identity. A family provides a microcosm of the wider society, with opportunities to learn and to practice these skills safely, and to receive guidance and feedback as they are being learned.
At any point in the child’s life these dimensions will be specific and possibly different, and interact with the child’s age, history, temperament, resources, history, handicaps, intelligence, attachment style.
- (vii)
-
Supportive social environment
The social ecological model (Bronfenbrenner 1979) considers behaviour from the perspective of continuous interactions within nested systems from individual, interpersonal, organisational, community, through to intercultural factors. In our child development focus these systems might be from the maternal dyad, father and sibling relationships, extended family and kinship group, family friends, school, neighbourhood, friends, church or sporting groups, work or shops, through to public services, the media and government. Parents need to facilitate their children’s development in the widening ripples from family intimacy towards social complexity.
Parents need a secure and social environment supportive to their important caregiving role. Within this nurturing environment an effective parenting team may consist of two parents, or one parent and significant support person, or a wider kinship parenting group. Their role is to mobilise and coordinate resources, to share skills and to support each other in the common parenting goal. Their capacity to share the tasks and responsibilities of parenthood is reflected in the higher educational, emotional and behavioural outcomes for children in families with two parents. Single parenthood is itself a risk factor for children, compared to the consistent presence of two parents, or parenting team. Similarly, a socially isolated family may not have the back-up resources to manage emergencies, provide guidance and help, and to enrich the social ecology around the child. Such a supportive network is often referred to as scaffolding. It is important to understand the specific parental resources supported by the family’s social ecology (eg back up physical care and babysitting, emotional support allowing the parents better affect management and hence emotional availability, a network that supports behaviour management and social learning), and also to consider the sustainability of this positive social ecology.
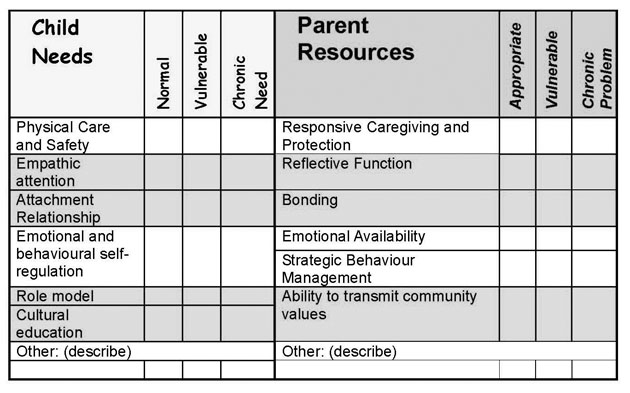
The diagram below attempts to show how a clinician may attempt to compare a child’s assessed needs to the assessed resources a parent may be able to offer. It can indicate areas of strength and weakness in the parent-child relationship, suggesting possible remediation interventions, and also allow explicit thinking about whether any necessary changes are viable.
References
Allerton M Assessment of Parenting Capacity, 2012.
Bonomi AE et al “Health care utilization and costs associated with childhood abuse” (2008) Journal of General Internal Medicine 23(3), pp 294–9.
Brennan J Assessment of Parenting Capacity. talk given to DoCS psychologists at Parramatta, 1996.
Bretherton I “Emotional availability: an attachment perspective” (2000) Attachment and Human Development 2(2), pp 233–241.
Bronfenbrenner U The ecology of human development Harvard University Press, Cambridge, MA, 1979.
Carr S and Francis A “Childhood maltreatment and adult personality disorder symptoms in a non-clinical sample” (2009) Australian Psychologist 44, pp 146–155.
Conroy E et al “Child maltreatment as a risk factor for opioid dependence: comparison of family characteristics and type and severity of child maltreatment with a matched control group” (2009) Child Abuse & Neglect 33(6), pp 343–352.
Crittenden PM “Dangerous behavior and dangerous contexts: a thirty-five year perspective on research on the developmental effects of child physical abuse” in Trickett P (ed) Violence to Children American Psychological Association, Washington DC, 1998, pp 11–38.
Crittenden PM Raising parents: attachment, parenting and child safety Willan Publishing, Cullompton UK, 2008.
Donald T and Jueridini J “Parenting capacity” (2004) Child Abuse Review 13 pp 5-17.
Fonagy P, risk and protective factors within early development, as linked to social inequalities (personal communication) 1998.
Fonagy P “Attachment, Reflective Function, Conduct Disorders and Violence” at <www.psychol.ucl.ac.uk/psychoanalysis/zipped/sanfrancisco.rtf>, 2000.
Kerr MA Black MM and Krishnakumar A “Failure-to-thrive, maltreatment and the behavior and development of 6-year-old children from low-income, urban families: a cumulative risk model” (2000) Child Abuse & Neglect 24(5) pp 587–98.
Lamont A Effects of child abuse and neglect for children and adolescents National Child Protection Clearinghouse, Australian Institute of Family Studies, 2010.
Lauretti A, Loding B “The evaluation of parental fitness in termination of parental rights cases: a functional-contextual perspective” (1998) Clinical Child and Family Psychology Review 1 pp 77–100
Martin HP (ed), “The abused child: a multidisciplinary approach to development issues and treatment”, Ballinger Publishing Company, Cambridge MA, 1976.
McLewin LA and Muller RT “Attachment and social support in the prediction of psychopathology among young adults with and without a history of physical maltreatment” (2006) Child Abuse and Neglect 30 pp 171–191.
Mrazek D, Mrazek P and Klinnert M “Clinical assessment of parenting” (1995) Journal of the American Academy of Child & Adolescent Psychiatry 34(3) pp 272–282
NSW Child Death Review Team 1999-2000 Report, NSW Commission for Children and Young People, Sydney, 2000.
Schore, AN Affect dysregulation and disorders of the self, The Norton Series on Interpersonal Neurobiology, WW Norton & Company, New York, 2003.
Steele BF and Pollock CB “A psychiatric study of parents who abuse infants and small children” in Helfer R and Kempe CH (eds) The Battered Child, 2nd ed, University of Chicago Press, Chicago, 1974, pp 80–133.
Stafford BS and Zeanah CH, “Attachment disorders” in Luby, JL (ed) Handbook of preschool mental health: development, disorders, and treatment, The Guilford Press, New York, 2006.
Steinhauer P The least detrimental alternative: a systematic guide to case planning and decision making for children in care University of Toronto Press, Toronto ON, Canada, 1991.
Wyndham, A, (personal communication) 2008.
1This article is adapted from a talk given to the NSW Children’s Court magistrates at a Judicial Commission s 16 Conference on 3 March 2010.
2Director Children’s Court Clinic, 12 December 2012.
3Eg Bonomi et al, 2008.
4Ibid.
5Kerr, Black and Krishnakumar, 2000.
6Carr and Francis, 2009.
7Conroy et al, 2009.
8Bonomi et al, 2008.
9McLewin and Muller, 2005; attachment security predicted levels of psychopathology irrespective of levels of physical maltreatment.
10Lamont, 2010.
11Martin, 1976, p 17.
12When I was supervising the Community Services Southern Regional Developmental Disability Psychologists, we reviewed the main resources describing developmental milestones (by Griffiths, Denver, Sheridan, Cooey and a Down Syndrome book).
13From Purdue Calumet’s School of Education website.
14Surveys were done in relation to assessments of 1564 children, and 2051 adults (1235 parents) assessed by the Children’s Court Clinic between January 2007 and July 2008.
15Allerton, 2012.